THE LIVING MATRIX BY MICHAEL KERN D.O., B.C.S.T., A.B.D., N.D.
“This philosophy has chosen the fascia as a foundation on which we stand … By its action we live and by its failure we die … The soul of man with all the streams of pure living water seems to dwell in the fascia of his body.”
- Dr. A. T. Still
Until recently fascia was largely ignored by anatomists. In dissections it was treated as the wrapping that needed to be cut through and discarded before getting to the interesting stuff. It has therefore been called the “Cinderella tissue”, because it’s often been neglected. However, in recent years some “fascia-nating” discoveries have been made:
- Fascia is an important element within a body-wide tensegrity system — ref. Donald Ingber and Dr. Stephen Levin
- Fascia is a liquid crystalline matrix — ref. Dr. Mae Wan Ho
- The insides of cells are connected to the outside via the fascial matrix — ref. Dr. James Oschman
- Fascia can contract independently of muscular activity and expresses a slow rhythmic motion — ref. Boris Hinz and Helene Langevin
- Fascia acts as a communication system — ref. Dr. Mae Wan Ho, Fritz Popp, Dr. James Oschman and Helene Langevin
- Fascia has a rich nerve supply and can transmit pain — ref. Robert Schleip and Dr. Jaap van der Wal
- Mechanoreceptors found in fascia have a direct influence on the autonomic nervous system — ref. Robert Schleip and Ernst Gellhorn
- Fascia can harden, de-hydrate, inflame and thicken — ref. Leon Chaitow, Helene Langevin and Robert Schleip.
Interestingly, many of these discoveries correspond to insights made by Dr. Andrew Still, the founder of osteopathy, more than 100 years ago. Below is a summary of these findings.
Fascial function
One of the basic principles of craniosacral work is that everything in the body is connected to everything else. As Dr. Still expressed, “The body is a unit of function” (Still, 1899). The fascia is a vital element within this integrated system. There is a continuous network of fascia from head to toe, and from the core of the body to its periphery.
Fascia is also an organ of support that helps to compartmentalise the different body structures. There is a superficial layer of fascia that immediately underlies the skin, and deeper layers (deep fascia and subserous fascia) that surround all the internal structures of the body. Each nerve, muscle, bone, vessel, gland and organ of the body is surrounded by deep fascia — as is each individual nerve fibre, muscle fibre and each group of fibres. In fact, every everything in the body is surrounded by fascia. If you took away all of the internal substance of the body, you would be left with a cast of each body part made of fascia. The musculoskeletal, cardiovascular, nervous, visceral and lymphatic systems all lie within the fascial system. The surrounding fascia determines the space used by the internal structures of the body, and so maintains their shape.
Fascial motility and adaptability
According to Dr. Jaap van der Wal, fascia is continuous with muscles and bones throughout the body, not just attached to them. This continuity of fascia with other elements of the musculoskeletal system can be attributed to their embryological origin in the mesoderm (van der Wal, 2009). In this way, fascia helps all areas of the body to work together in coordinated patterns of movement.
In health, all the fascial compartments throughout the body move in reciprocal relationship. The fluid found within and between the fascial sheets helps to reduce any friction so that this motion can more easily occur. Fascial motion takes place during our more pronounced voluntary and involuntary movements, and during our subtle primary respiratory motion. It allows for each part of the body to move against its neighbour, and accommodates for the inner breathing or motility of the organ or structure it contains. When there is no resistance provided by their surrounding fascia, all tissues have room to express primary respiration and are therefore able to express their original matrix of health.
Cells, and in particular mesodermal cells, have a wide ability to respond to a changing environment. Mesoderm contains types of non-specific cells that give rise to specialised cells as needed during our embryological development. Furthermore, mesodermal cells guide the embryological development of different organs. As long as liver cells stay inside their mesodermal surrounding during development, this environment will determine that they become liver. Potential pancreatic cells do not differentiate into mature pancreas unless they are in a specific mesodermal environment (potential fascia). This environment may provide the specific energy field required for this tissue to form (Schulz and Feitis, 1996).
Liquid Crystalline Matrix
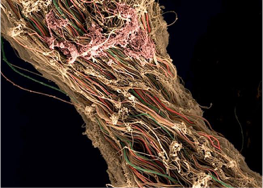
Fascial tissue basically consists of two components: cells and the extracellular matrix (Klinger and Schleip, 2015). Unlike most other tissues, the cells take up a minor part of the total volume (usually less than 5%). Most of the cells are fibroblasts, which are involved in the construction and maintenance of the surrounding matrix. The matrix itself consists of two parts: an abundant fluid ground substance and fibres. The fibres consist mostly of collagen fibres meshed together in sheets, as well as a few elastin fibres.
The hollow collagen fibres also contain fluid and make up 70% or more of all the proteins of connective tissues. Collagen is therefore the most abundant protein in the body. The fluid ground substance can vary in density from being quite watery to having a thicker, more gel-like state. A variety of different tissue types are formed, dependent on the fluidic nature of the ground substance, and the quantity and arrangement of collagen and elastin fibres.
It has been demonstrated that small amounts of cerebrospinal fluid (C.S.F.) seep out from the spinal core along with the spinal nerves that exit at each vertebral segment, as well as in the olfactory nerves that pass through the ethmoid bone. The hollow collagen fibres in the surrounding connective tissue are considered to be the agency by which this occurs, helping to transport C.S.F. into the rest of the body. This supports an original hypothesis by Dr. Sutherland, that cerebrospinal fluid potentises the whole body. Through its internal network of collagen fibres, the fascia can be seen as one of the mechanisms by which the potency of the Breath of Life is conducted throughout the body.

Interestingly, the fluidic ground substance in fascia has a similar composition to C.S.F. Like C.S.F., this fluid also expresses tide-like rhythmic motions. Claire Dolby D.O. remarks, “In the cranial concept, at a core level cerebrospinal fluid expresses the potency of the Breath of Life within the dural membranes. In the whole body, interstitial and lymphatic fluids at a cellular level and a tissue level carry out this role.”
The collagen fibres within fascia are organised in the shape of a triple helix; i.e. a spiral. Due to this architectural configuration, there is a spiral motion within the fluid and potency that moves through the fascia (Wilks J. and Knight I., 2014). Spiral motion is a common feature in biological systems. According to Austrian forester and inventor Viktor Schauberger, spiral movement patterns in nature provide the capacity for generating and transmitting life-giving forces.
Dr. Mae Wan Ho describes fascia as a “liquid crystalline matrix”, an organic crystalline tissue that functions between a fluid and solid state (Ho and Knight, 1998). In healthy fascia, a large percentage of the extracellular fluid is in a state of ‘bound water’ (as opposed to ‘bulk water’). Bound water has a negative electrical charge, which is considered important for healthy biological systems (Pollack, 2001). Much pathology, such as inflammatory conditions or the accumulation of waste products, tends to go along with a shift towards a higher percentage of bulk water within the ground substance.
Fascial hydration generally decreases with under-use and in old age. Deane Juhan describes dehydrated and stuck fascial tissues as “thixotrophic” (Juhan, 2002). Indications by Sommer and Zhu (2008) suggest that when fascia gets squeezed like a sponge and subsequently rehydrated during exercise, some of the previous bulk water zones may then be replaced by bound water molecules. Dr. Still observed, “This connecting substance [fascia] must be free at all parts to receive and discharge all fluids, and use them in sustaining animal life, and eject all impurities, that health may not be impaired by dead and poisonous fluids” (A.T. Still, 1902).
In Craniosacral practice, we work with the intimate relationship between fluid and potency. Potency loves fluid and vice versa — where one goes, so does the other! We know that fluid acts as the carrier of life, but it’s also found that the expression of potency within the body directly influences fluid dynamics. Fluid re-hydration naturally occurs when potency is re-established. Therefore, if we are able to facilitate the expression of potency in the body (e.g. by resolving inertial fulcra or augmenting primary respiration), the tissues can naturally re-hydrate.
Fascia As A Communication System
Fascia is seen as a communication system for whole the body (Oschman, 2012; Ho and Knight, 1998). Dr. Mae Wan Ho describes this liquid-crystalline matrix as being highly responsive to electrical charge, and also able to carry impulses very fast. She suggests that impulses created in the fascia are amplified via the action of proteins in the liquid crystal.
The collagen fibres in fascia have been described as the conductor of electrons in the body, whilst the ground substance is the reservoir of electrons (Oschman, 2008). Dr. Zvi Karni, a professor of Biological Engineering in Israel, has also demonstrated that fascia is able to conduct electricity, so helping to transmit energy throughout the body and act as a carrier of information (Upledger and Vredevoogd, 1983). Furthermore, the collagen fibres can transmit photons (light) and have been measured to have piezoelectric properties (the ability to generate an electric charge in response to applied pressure). The collagen fibres can be thought of as “fibre optics” for the body, in which impulses can be created by very light pressures. The conductivity of collagen is dependent on how hydrated it is; the more hydrated, the more impulses can flow freely through the fascia.
Herbert Frohlich (1968) and Fritz Popp (2003), have demonstrated that living cells emit light (photons) across a wide variety of wavelengths and that this is an important way in which cells communicate with each other. According to Dr. Will Wilson, “In cancer the output of light is much reduced, thereby reducing the potential for cell-to-cell communication. Cancer cells act as if out of touch with the rest of the organism, proliferating uncontrollably. So, for cellular health it seems likely that a light-based communication system is needed”. Dr. Sutherland talked about liquid light and transmutation, so perhaps he was describing from observation what science is now starting to explain in the language of biology (Ukleja, 2012).
The connective tissue matrix can pick up low-level signals, much of which never goes to the brain. A huge amount of information pours through the connective tissue matrix, which acts as an antenna picking up information from both inside and outside the body. This produces subtle “whispers” within the body physiology. The nerves within the body can just pick up the tip of the iceberg, as they only become activated by certain strong stimuli (Oschman, 2008). If this principle is applied in clinical practice, it can mean that “less is more”; small amounts of energy can have large effects and doing less can have a greater effect. Very pertinently for Craniosacral Biodynamics, here is Dr. Mae Wan Ho’s observation about living organisms, “Coherent energy is stored everywhere within the system … Consequently any subtle influence arising anywhere within the system will propagate over the entire system and get amplified to global effects. In other words, the system, by virtue of being full of coherent energy everywhere, will be ultra-sensitive to very weak signals. This may be the basis of all forms of subtle energy medicine” (Ho, 1998).
The whole fascial matrix has been described as an information superhighway, that has links with the nervous system, enables inter-cellular signalling and supports high speed interchange at a molecular level. The nervous system has traditionally been considered as an extremely fast communication system, but in comparison to the high speed communication that takes place within the fascial matrix it is positively sluggish! According to Dr. Mae Wan Ho, the nervous system is actually designed to slow things down to help regulate body functioning. According to Ho, “Liquid crystallinity gives organisms their characteristic flexibility, exquisite sensitivity and responsiveness, and optimizes the rapid noiseless intercommunication that enables the organism to function as a coherent coordinated whole” (Ho, 1998). According to Katherine Ukleja, working intelligently with the liquid-crystalline nature of the connective tissue matrix means much more than simply resolving muscular-skeletal strains. It is a wonderful opportunity to alter body physiology at a cellular and molecular level.
Tensegrity
Fascia is part of a tensegrity system in which all elements are held in a state of reciprocal tension. In tensegrity structures, any pull or movement in one area will be transmitted and accommodated for within the whole system. Dr. Stephen Levin, an orthopaedic surgeon, coined the phrase ‘biotensegrity’ to describe the application of tensegrity principles to biological systems. Tensegrity can be used to explain the complex interaction that maintains our structural homeostasis. Donald Ingber, a pioneering scientist who works with the biological application of tensegrity, describes the role payed by fascia as, “A system that stabilises itself mechanically because of the way in which tensional and compressive forces are distributed and balanced within the structure” (Ingber, 1998).
In tensegrity structures none of the rigid structures touch each other and often appear to hang in space as though unsupported. In the body, joints provide the spaces for these structures. This marks a significant conceptual shift from the view that our bones are load bearing structures, like the framing of a house. Levin points out that if our bones acted as a system of ‘compression members’, like the beams and rafters in a house, then the force of regular daily loads would result in a shearing and crushing of our bones. Rather it is the ‘tensional members’, the muscles, fascia, ligaments and tendons, which can account for our ability to perform everyday tasks. Compressive forces only become taken up in the joint spaces in states of mechanical strain and pathology. As Louis Schulz observes, “Bones are spacers, serving to position and relate different areas of the connective tissue. Bones are not the supporting structures of the body; the connective tissue serves this function” (Schulz and Feitis, 1996).

Fascia has the properties of being pliable and tough. Until recently it was also considered to be inelastic, but research now shows the presence of highly contractile fibres called ‘myofibroblasts’. Myofibroblasts are the ‘building block’ cells of fascial tissue and they play an important role in maintaining fascial tension. It has been found that these cells have contractile characteristics of smooth muscle (Levin and Martin, 2012) and can become affected in many kinds of connective tissue disorders such as frozen shoulder and low back pain.
Research by Robert Schleip suggests that fascia can contract independently of muscular action and thus actively influence muscle dynamics (Schleip, Klingler and Horn, 2005). Furthermore, an important property of fascia is its ability to recoil, which plays a significant role in efficient movement. This has been demonstrated in the denser sheets of fascia, such as the thoracolumbar fascia (Wilks J. and Knight I, 2014). A good spring-like recoil is dependent on good hydration within the fascia.
Very interestingly for our work, experiments have also shown that myofibroblasts exhibit a steady rhythmic motion that has been measured at 100 second cycles when placed in a collagen-based matrix (Follonier et al, 2010). This slow motion corresponds to the long tide described by biodynamic craniosacral practitioners (Kern, 2005).
The Living Matrix
Dr. James Oschman describes fascia as a central element within a living matrix, a material and energetic substrate that is involved in tissue organisation, communication and repair. The living matrix connects all the functions in the body and can also be compared to the operating system that connects all the functions of a computer, such as the keyboard, screen, modem, programmes, etc. (Oschman, 2008).
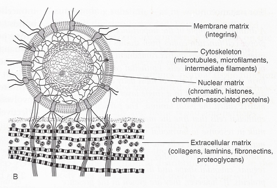
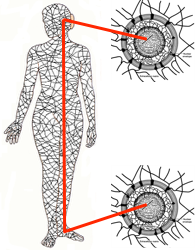
Within the living matrix, the meshwork in the extra cellular matrix (ECM) extends to the inside of each cell through micro-filaments of the cytoplasm, right up to the cell nucleus (Oschman, 2008). This understanding extends the principle of tensegrity to include the structures inside the cell, which become part of the tensegrity network. It also means that every cell is in touch with every other cell in the body.
The bridge between the ECM and the cell cytoplasm is provided by integrins. According to Flores and Patel (quoted in Ukleja, 2012), “Integrins are the principal receptors used by animal cells to bind to the extracellular matrix … Integrins also function as signal transducers, activating various intracellular signalling pathways when activated by matrix binding. Integrins and conventional signalling receptors often cooperate to promote cell growth, cell survival, and cell proliferation”.
Transduction refers to the action of converting something (especially energy or a message) into another form. So, signal transduction from the outside to the inside of the cells is carried out by integrins. Integrins respond to mechanical cues. This means that cells communicate with other cells by pulling on each other’s membranes and distorting the cytoplasm. Scientifically this process is called ‘mechanotransduction’.
Donald Ingber writes, “Mechanotransducers are molecules that change their chemical activity state when they are mechanically distorted, and thereby convert mechanical energy into biochemical energy … the function of virtually every molecule could potentially be altered by mechanical stress because all bioactive molecules move between extended and contracted forms … in the process of carrying out their biochemical activities” (Ingber, 2005). According to Ingber, it is becoming increasingly clear that epigenetic factors, particularly mechanical and structural cues that influence cell behaviour, have a central role in embryogenesis and tissue physiology (Ingber, 2005).
Due to the continuity of the ECM with the liquid crystalline cytoplasm in the interior of cells, everything everywhere in the body is in communication via this continuum. Remember that impulses can travel through this network at high speed; probably at the speed of light. However, distortions, inertia, and loss of hydration can effect the conduction of these impulses. This may be an important cause of fragmentation of function between different parts of the body. Furthermore, as the ECM in fascia connects into cytoskeleton of cells and in turn the cytoskeleton connects into the cell nucleus, any tension in fascia is now known to affect the expression of DNA in the nucleus.
Fascia And The Nervous System
Dr. Andrew Still wrote in 1902, “No doubt nerves exist in the fascia” and suggested that fascia should be treated with the same degree of respect as if dealing with “the branch offices of the brain” (Still, 1902). Dr. Jaap van der Wal reported in 1988 the presence of substantial nerve endings in the fascia of rats, but his finding was ignored for decades (van der Wal, 1988). However, in 2007 three teams from different countries independently reported findings of a rich presence of sensory nerves in fascial tissues (Findley and Schleip, 2007).
The fascial tissue surrounding nerve fascicles (the perineurium) and that surrounding the whole nerve and associated veins and arteries (the epineurium) play important roles in pain regulation. Bove and Light (2008) conducted studies revealing nerve axons in the epineurium and perineurium that are consistent with nociceptive (pain) function. Subsequent studies using in vitro electrical and chemical nerve stimulation demonstrated that stimulation of local nociceptive receptors of the perineurium and/or epineurium can evoke nerve inflammation. This indicates that irritation of perineural fascial tissues can trigger local nerve inflammation and pain. Evidence indicates that chronic low back pain may actually emanate from fascia, rather than bone, cartilage, or musculature. Subsequent work has also implicated lumbar fascia as well as peri-spinal ligaments as common culprits of low back pain. Thomas and Robet (2009) found corroborating histological evidence indicating that low back pain may be due to inflammation in the lumbar fasciae. Indeed, the magnitude of low back pain often does not correlate with the magnitude of disc displacement or degeneration.
Fascia is now actually considered to be the most richly innervated tissue in the body, with a very high density of sensory nerves; in particular proprioceptors that help our nervous systems to orient to our surroundings. Additionally, with regards to sheer quantity and richness of nerve endings, this network can ‘match’ our sense of sight, not to mention hearing or any of our other normally considered sensory organs (Schleip, 2015). Fascia monitors and constantly responds to what’s going on in our surroundings and where we are in space. The fascial web can be seen as our largest sensory organ in terms of overall surface area.
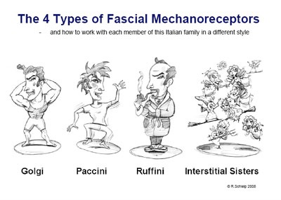
Mechanoreceptors
There are key mechanoreceptors within the fascia, as well as in subcutaneous tissue, membranes and tendons. These are:
Golgi receptors — found in deep fascia, ligaments and myo-tendinous junctions. These are involved in proprioception and respond to deeper pressures and strong stretches only.
Pacini receptors — found in myotendinous junctions, deep joint capsules, spinal ligaments and surrounding muscular tissues. These are also involved in proprioception. They respond to sudden pressures and rhythmic movements such as shaking and rocking.
Ruffini receptors — found in the skin, dural membranes, ligaments and joint capsules. These are also involved in proprioception, and they respond to slowly-applied pressures and stretching. They are able to create a global relaxation response by decreasing sympathetic tone in the whole body. Ruffinis also change local fluid dynamics and aid tissue metabolism.
Interstitial receptors (“type III and IV”) — these are widespread in the body and are the most abundant receptors found in fascia. They are located almost everywhere in the body, even inside bones, with a high density found in the outer periosteal layers of bones. Some of these receptors are high-threshold, but about 50% are low-threshold fibres that respond to very light touch and to very subtle stimulation (Wilks J. and Knight I., 2014). Furthermore, many receptors of interstitial nerves are responsive to more than one kind of stimulation (Schleip, 2015). Robert Schleip and his team have also established that the innumerable small caliber nerves abundantly found in fascia that were previously thought of solely as pain fibres (nociceptors), are in fact interstitial mechanoreceptors with a much wider function.
When stimulated, the interstitial receptors increase vagal tone and consequently decrease sympathetic nervous system activity. Interstitial receptor stimulation leads to a change in heart rate, blood pressure regulation and lung respiration. Some interstitial receptors are also involved with thermo-reception, and can help regulate blood flow to muscles by monitoring muscular activity to the sympathetic nervous system (Schleip, 2015). Schleip reports, “It seems that a major function of this intricate network of interstitial tissue receptors is to tune the nervous system’s regulation of blood flow to local demands, and this is done via very close connections with the autonomic nervous system” (Schleip, 2003).
Robert Schleip notes that slow and gentle contacts generally stimulate an increase in the parasympathetic nervous system, with an increase in vagal tone, and thus facilitate the calming of emotional states (Schleip, 2003). This type of contact activates the anterior lobe of the hypothalamus and has the effect of lowering muscle tonus throughout the body, producing cortical and endocrinal changes that are associated with deep and healthy relaxation (Ernst Gellhorn, 1967). To put it simply: any intervention on the fascia is also an intervention on the autonomic system (Ukleja, 2012).
Interstitial receptors can function both as mechanoreceptors (responding to mechanical tension and/or pressure) and as pain receptors. In the presence of pain, their sensitivity changes so that normal physiological pressures can lead to strong and chronic firing of these receptors. This explains why pain often exists without any mechanical irritation of nervous structures, as was frequently assumed by the nerve root-compression model (Chaitow and DeLany, 2000, quoted in Schleip, 2003).
Fascia plays a big role in delayed muscle soreness after exercise. If over-sensitised, the interstitial receptors can be involved in situations of chronic pain and sensitivity. This can lead to the existence of pain without mechanical irritation of nervous structures (Liptan, 2010). Chronic inflammation can be one cause leading to the hyper-sensitivity of nociceptors. Treatment that employs a soft touch, and that does not consequently elicit a pain response, can be very helpful in helping to break these cycles of pain and inflammation.
The interstitial nerves in fascia also serve an interoceptive function. This provides the brain with information about the internal condition of the body, such as warmth, nausea, hunger, soreness, effort, heaviness or lightness, as well as a sense of belonging or alienation regarding specific body regions (Craig, 2002).
Schleip concludes, “Our richest and largest sensory system is not the eyes, ears, skin, or vestibular system but is in fact our muscles with their related fascia. Our nervous system receives its greatest amount of sensory input from our myofascial tissues. Yet the majority of these sensory neurones are so small that until recently little has been known about them” (Schleip, 2003).
CLINICAL APPLICATIONS: FASCIAL FUNCTION
“I know of no part of the body that equals the fascia as a hunting ground.”
- Dr. A.T. Still
Inertial fulcra distort the fluid/tissue matrix and can effect its many functions. During palpation these conditioned patterns may be felt as as a drag or pull through your hands, organised around an inertial fulcrum. Or, they may be sensed as subtle distortions within the whole field of tissues, fluid and potency as primary respiratory motion is expressed three-dimensionally around the presence of an inertial fulcrum.
If the practitioner can support the client to settle into a holistic shift (patient neutral), an automatic shifting of potency can begin to move towards the fulcrum that’s ready to be worked with. This can be facilitated by the practitioner sitting back with an orientation to the whole field of tissues, fluid and potency of the client, and not following the first patterns that show themselves. The holistic shift is essentially a state of settling and letting go, in which the client is sufficiently safe and resourced so that they are able to stop managing or controlling what’s going on during a session. It marks a physiological shift from a sense of fragmentation and conditioned motion patterns to a sense of wholeness and connection to resources. It is the gateway to a deeper therapeutic process, in which there can be a resolution of the forces organising an unresolved pattern.
Craniosacral biodynamic treatment skills, such as synchronising to expressions of Primary Respiration, accessing states of balance and/or employing augmentation skills, can be used to re-orient the pattern imprinted in the fascia to our underlying matrix of health and wholeness.
The light touch, synchronised to the needs of the patient, used in Craniosacral practice may have the following effects:
- Increase the expression of potency through the fascial matrix
- Re-establish a connection with the wider matrix of Health (Primary Respiration)
- Support the hydration of myofascia
- Stimulate mechanoreceptors in fascia (particularly some interstitial receptors and possibly Ruffinis)
- Increase vagal tone and lower the stress response
- Stimulate efficient blood supply
- Help to re-establish fascial contractility and recoil
- Facilitate greater coordination of movement within the body
- Improve organ function
- Reduce pain and inflammation
- Facilitate greater interoceptive awareness
- Assist with local and global cellular function
- Facilitate light-based and electrical communication throughout the body.
REFERENCES:
Bove G. and Light A. (2008) Epi-Perineurial Anatomy, Innervation, and Axonal Nociceptive Mechanisms. Journal of Bodywork and Movement Therapies, 12(3): 185–190.
Chaitow, L (1980) Soft Tissue Manipulation. Thorsons, Wellingborough.
Craig, A.D. (2002) How do you feel? Interoception: the sense of the physiological conditioning of the body. Nat Rev Neuroscience 3(8): 655–666.
Findley T., Schleip R. (eds.) 2007 Fascia Research — Basic science and implications conventional and complementary healthcare. Elsevier Urban and Fischer, Munich.
Gellhorn E. 1967 Principles of autonomic-somatic integration: physiological
basis and psychological and clinical implications. University of Minesota Press.
Giumberteau J-C. (2005) Strolling Under The Skin: Images of Living Matter Architectures. Film directed by Giumberteau J-C.
Guimberteau J-C. and Bakhach J. (2007), A fresh look at vascularized flexor tendon transfers: concept, technical aspects and results. Journal of Plastic, Reconstructive and Aesthetic Surgery 60,793–810.
Follonier C. et al (2010) A new lock step mechanism of matrix remodeling. Journal of Cell Science 123, 1751–1760.
Frohlich H. (1968) International Journal of Quantum Chem 2: 641–49.
Ho M-W (1998) Coherent Energy, Liquid Crystallinity and Acupuncture. American Journal of Chinese Medicine 26.
Ho M-W. and Knight D. (1998) The acupuncture system and the liquid crystalline collagen fibres of the connective tissues. American Journal of Chinese Medicine 26 (3–4), 251–253.
Ingber D.E. (1998) The architecture of life. Scientific American 278, 48–57.
Ingber, DE. (2005) ‘Cellular mechanotransduction: putting all the pieces together again’. The FASEB Journal Vol 20, Issue 7, 2–4.
Klinger W. and Schleip R. (2015) Fascia as a body-wide tension network: anatomy, biomechanics and physiology in Fascia: In Sport and Movement 5, Handspring Publishing.
Juhan D. (2002) Job’s Body — A Handbook for Bodywork. New York: Station Hill Press.
Kern M. (2005) Wisdom In The Body — The Craniosacral Approach to Essential Health. North Atlantic Books.
Langevin H.M. et al 2011. Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskeletal Disorders 2011, 12:203.
Levin S. and Martin D-C (2012) Biotensegrity: the mechnics of fascia. In R. Schleip et al (eds) The Tensional Network of the Human Body. Churchill Livingstone, Elsevier.
Liptan, G.L. (2010) Fascia: A missing link in our understanding of the pathology of fibromyalgia. Journal of Bodywork and Movement Therapies,
2010 Jan;14(1): 3–12.
Oschman J. (2003) Energy Medicine in Therapeutics and Human Performance. Oxford: Butterworth-Heinemann.
Oschman J. (2008) Seminar at Craniosacral Therapy Educational Trust, London.
Oschman J. (2012) Fascia as a body-wide communication system. In Schleip R., Findley T.W., Chaitow L. and Huijing P. (eds) Fascia: The Tensional Network of the Human Body: The Science and Clinical Applications in Manual and Movement Therapy (1st Edition), Churchill Livingstone.
Pollack G.H. (2001) Cells, Gels and the Engines of Life. Ebner & Sons
Popp F. (2003) Properties of biophotons and their theoretical applications. Indian Journal of Experimental Biology, Vol 41, May 2003, 391–402.
Schleip R. (2003) Fascial plasticity — a new neurobiological explanation. Parts 1 and 2. Journal of Movement and Bodywork Therapies 7, 1, 11–19.
Schleip R. Ed. (2015) Fascia: In Sport and Movement. Handspring Publishing.
Schleip R. (2010) Hinweise Auf Eine Fasziale Rhythmikität, in Deutsche Zeitschrfte fur Osteopathie: 4/2010, Hippokrates Verlag
Schleip R., Kllinger F. and Horn F. (2005) Active fascial contractility: fascia may be able to contract in a smooth muscle-like manner and thereby influence musculoskeletal dynamics. Medical Hypotheses 65 (2), 273–277.
Schulz R.L., Feitis R. (1996) The Endless Web: Fascial Anatomy and Physical Reality. Berkeley, CA: North Atlantic Books.
Sommer A.P., Zhu D. (2008) From microtornadoes to facial reju-
venation: implication of interfacial water layers. Crystal
Growth and Design 8, 3889e3892
Still A.T. (1899) Philosophy of Osteopathy. Re-printed 2014: CreateSpace Independent Publishing Platform.
Still A.T. (1902) The philosophy and mechanical principles of osteopathy. Hudson-Kimberly Publishing Company, Kansas City, 61–62.
Thomas F. and Robet S. (2009), “Introduction,” in Fascia Research II, Amsterdam Basic Science and Implications for Conventional and Complementary Health Care, p.7, Elsevier Press, Amsterdam.
Ukleja K (2012) Fascia — new directions. Unpublished article and class notes at Craniosacral Therapy Educational Trust.
Upledger J. and Vredevoogd J. (1983), Craniosacral Therapy. Eastland Press 236
van der Wal J.C. (2009) The Architecture of Connective Tissue as a Functional Substrate for Proprioception in the Locomotor System. Amsterdam: Second International Fascia Research Congress.
van der Wal J.C. (1988) The organisation of the substrate of proprioception in the elbow region of the rat. [PhD thesis]. Maastricht University, Faculty of Medicine.
Wilks J. and Knight I. (2014) Using The Bowen Technique. Singing Dragon.
© Michael Kern 2015
